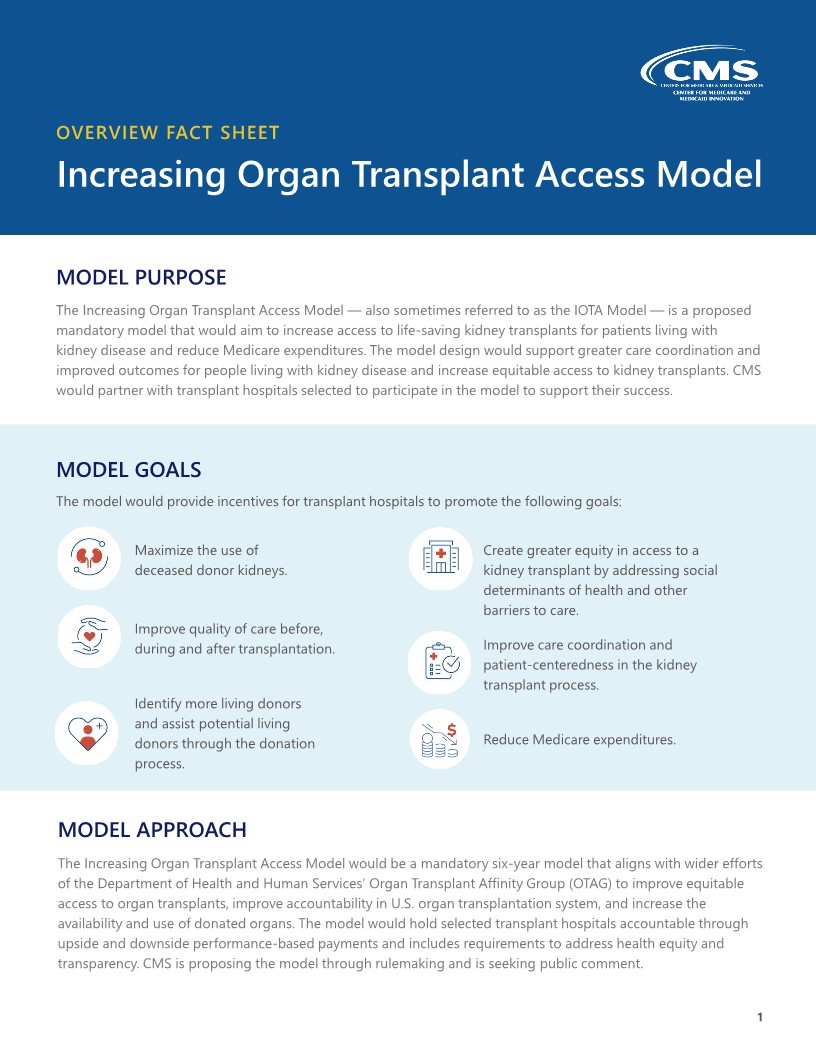
The CMS Innovation Center released an alternative payment model, Increasing Organ Transplant Access (IOTA), that will hopefully improve access to kidney transplantation, increase the number of kidney transplants, enhance living donation, require transplant centers to transparently share their transplant selection criteria, and also tell patients the reasons why organs are declined on their behalf.
The fact sheet for this MONUMENTAL win for kidney patients is attached. (Let’s discuss on our next call!)
HRSA is still focused on revamping the organ donation and transplant system with its Modernization Initiative to create a best-in-class Organ Procurement and Transplantation Network that works more efficiently on behalf of those who selflessly donate precious organs and individuals in need of life-saving transplants.
HHS has issued a directive to collect pre-waitlist data to examine inequities in the transplant referral and evaluation processes to close the disparity chasm— a long overdue action that is necessary to implement interventions to advance equity in kidney transplantation.
Healthcare is not a privilege it is a right. Every person deserves to have access to high-quality, affordable, patient-centered care.
HRSA is still focused on revamping the organ donation and transplant system with its Modernization Initiative to create a best-in-class Organ Procurement and Transplantation Network that works more efficiently on behalf of those who selflessly donate precious organs and individuals in need of life-saving transplants.
HHS has issued a directive to collect pre-waitlist data to examine inequities in the transplant referral and evaluation processes to close the disparity chasm— a long overdue action that is necessary to implement interventions to advance equity in kidney transplantation.
Healthcare is not a privilege it is a right. Every person deserves to have access to high-quality, affordable, patient-centered care.
Access the full PDF document here: https://www.cms.gov/files/document/iota-model-fs.pdf


 TransplantFirst Academy is raising community awareness in living kidney donation.
TransplantFirst Academy is raising community awareness in living kidney donation.